A Comment about Internet Pictures:
It is such a blessing to have access to images and videos to reinforce your education. There is a huge variation in people and viewing different images helps you understand that variation.
Nevertheless, many images are produces by people with little medical training. You should especially be skeptical of images that clearly come from Shutterstock, Getty images and the like. The best ones are from medical journals and those with really messy backgrounds.
A Note about Abnormal Findings:
Many physical exam maneuvers have notoriously low sensitivity and specificity. The information you gain from the physical exam must be placed in a larger context. The importance of an abnormal finding is very dependent on your pretest probability of something bad going on.
Often, an abnormal finding should prompt you to re-examine the same finding more closely and to look for additional findings more carefully.
For instance, not being able to palpate a dorsalis pedis pulse in either foot of a young adult with no complaints is probably more a reflection of your skill or their anatomic variation than it is of disease. However, it should prompt you to recheck for pulses: repositioning your fingers, trying a different location. However, it should also prompt you to check femoral pulses, which if diminished or absent, might prompt you to consider coarctation of the aorta, for example.
A finding of a palpable lymph node is not uncommon. However, a palpable lymph node should prompt you to more carefully examine it to evaluate its size, firmness, mobility, etc., and to check for other lymph nodes, such as axillary nodes.
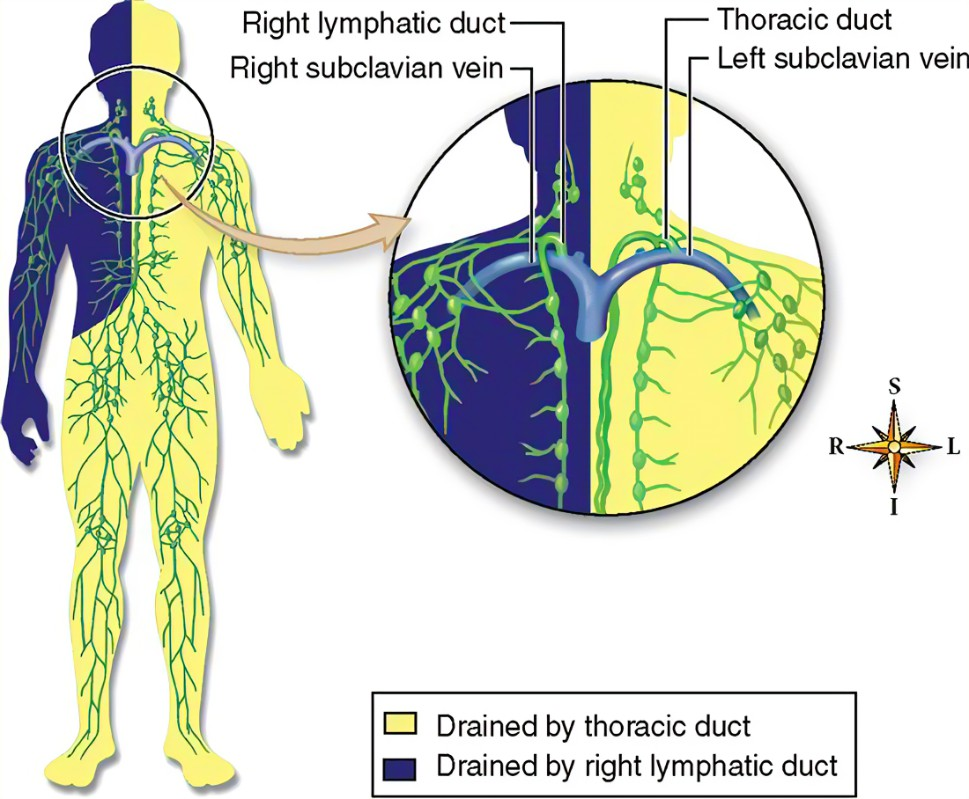
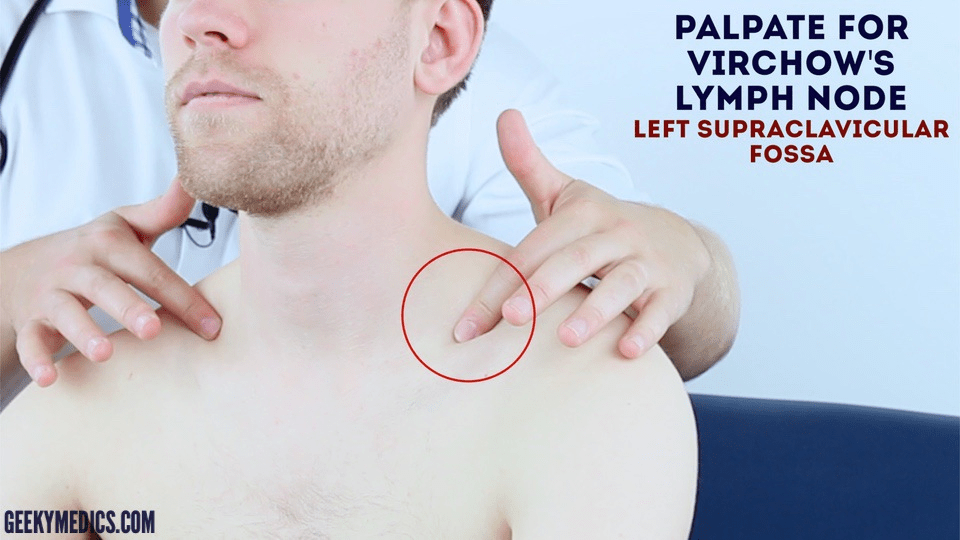
Supraclavicular lymph nodes
Any palpable lymph node in the supraclavicular fossa is abnormal. A Virchow node is specific for the left side because a large part of the body is drained by the lymphatic system going to the thoracic duct on the left. Classically, a Virchow node is considered a sign of gastric cancer or gastrointestinal cancer, but it can show up from any metastatic cancer in its drainage area. An enlarged lymph node in the right supraclavicular fossa is bad too; it just is less likely to be from a gastrointestinal cancer.
Lymph nodes (anywhere) will be palpable before they are big enough to see. Therefore, all pictures of lymph nodes show pretty good-sized lymph nodes.


Epitrochlear lymph nodes
We didn’t practice palpating epitrochlear lymph nodes, but you’ll need to know this at some point.


Epitrochlear lymphadenopathy is fairly rare but is classically associated with syphilis. It can also be seen in melanoma of the extremity or lymphoma.
Internal Jugular
I just want to remind you that the internal jugular vein lies under the sternocleidomastoid muscle. If you can clearly see the neck vein, it is the external jugular vein.

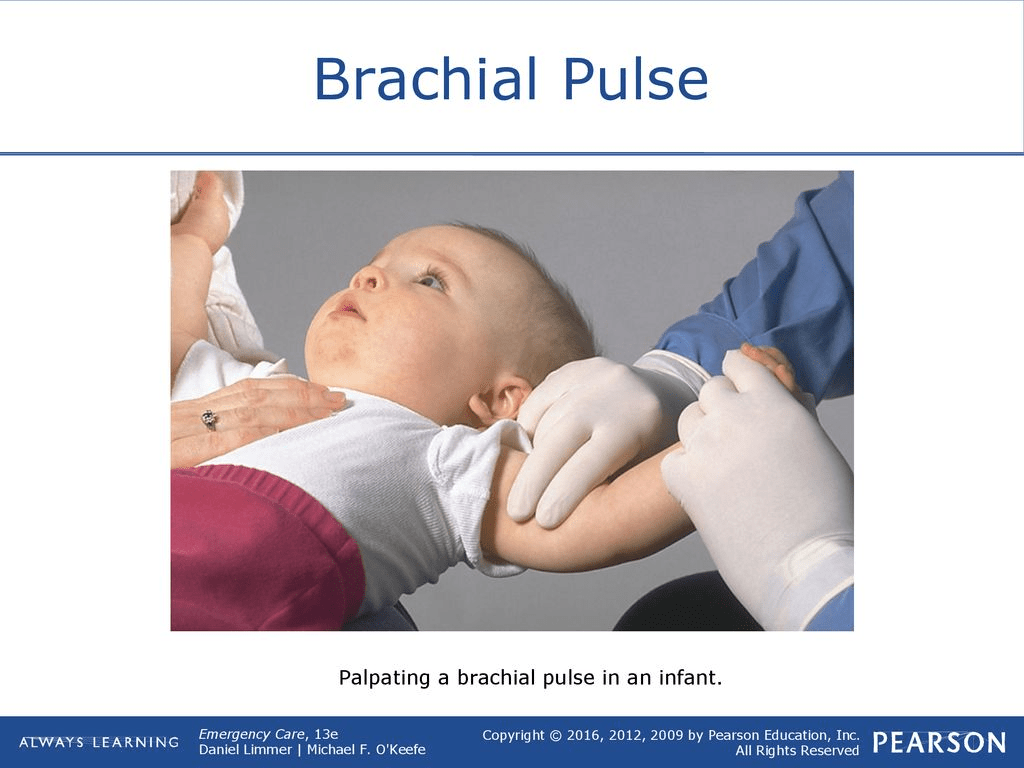
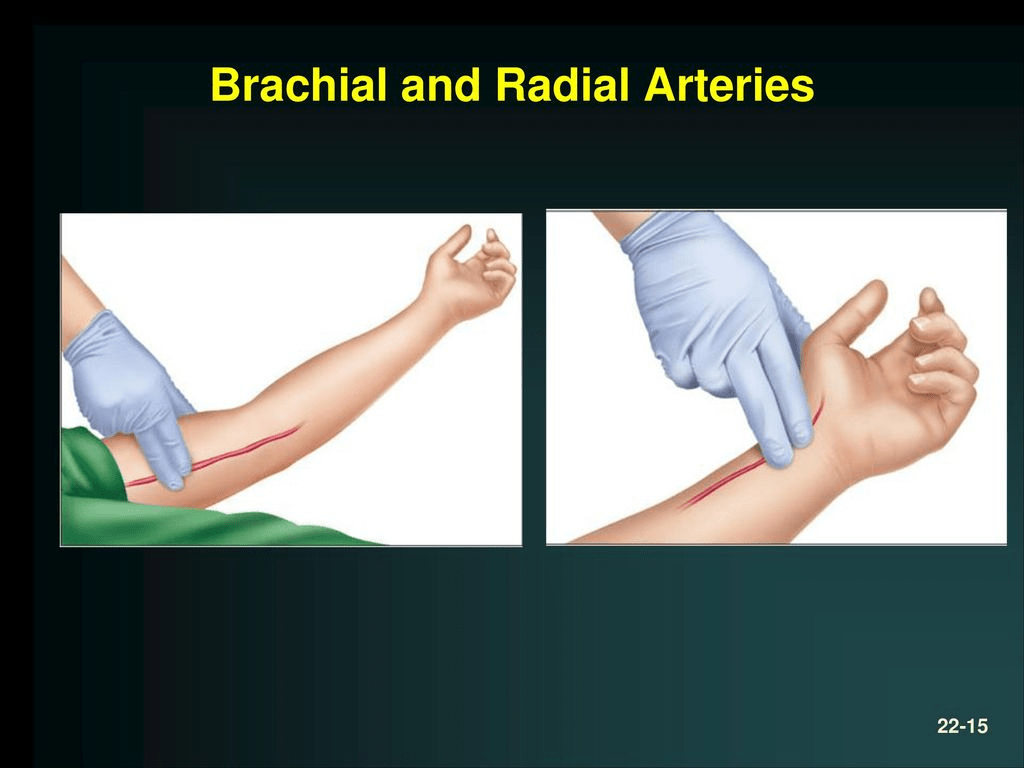
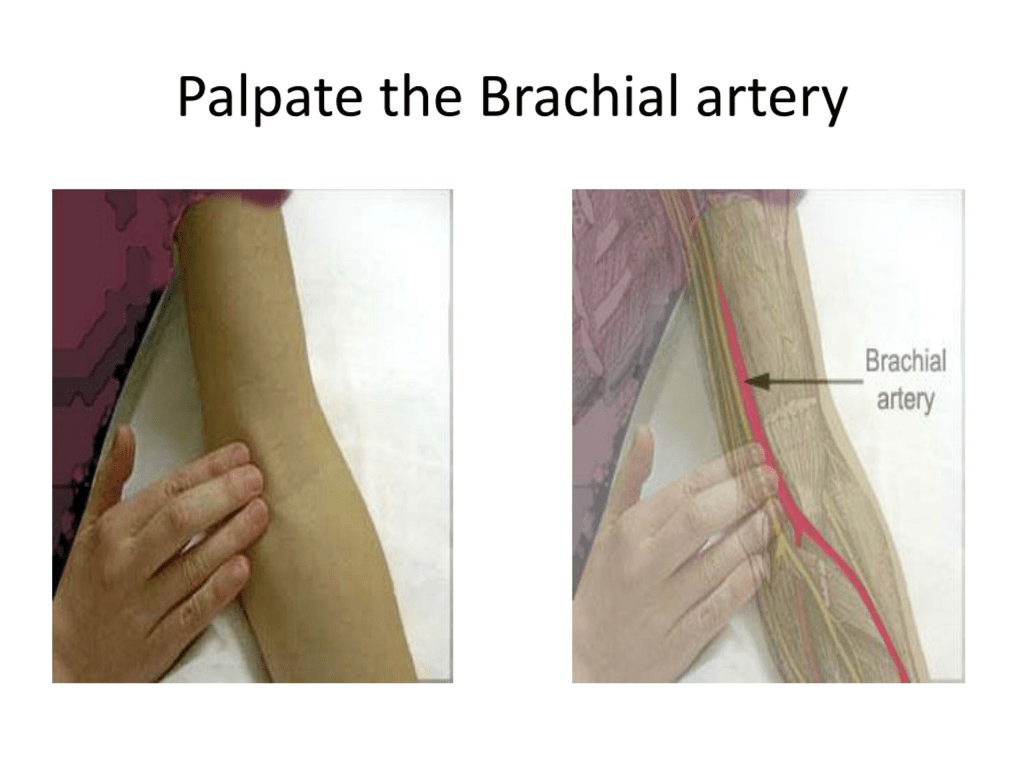
Brachial pulse
There are different places to feel the brachial pulse. Both of these places are feeling the pulse in the same artery. There are a few reasons to check a brachial pulse:
- this is the traditional place to check a pulse during infant resuscitation
- if you are accessing the vein in the upper arm and want to make sure you don’t hit the artery
- if you want to draw an arterial blood gas from the artery
- in a patient without a wrist
- when checking blood pressure
Personally, I check the brachial pulse about mid-arm on the medial side, pressing against the humerus. Partly, this is from my pediatric training and partly because this is where I feel it most easily on myself.
The important thing to know is that there are two options of locations to check and that if you don’t feel it in one location, it may be easier to feel in the other location.



Carotid pulse
The carotid pulse does not vary significantly. The important thing is that it is anterior to the sternocleidomastoid muscle.

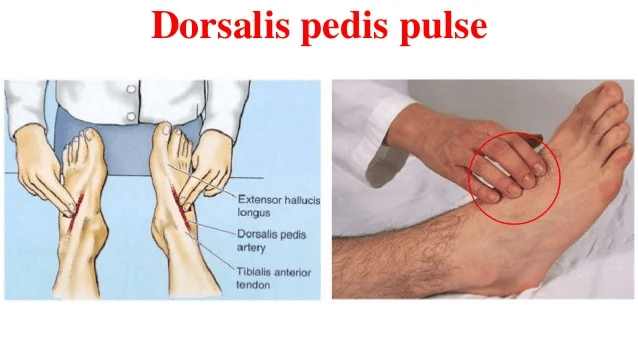
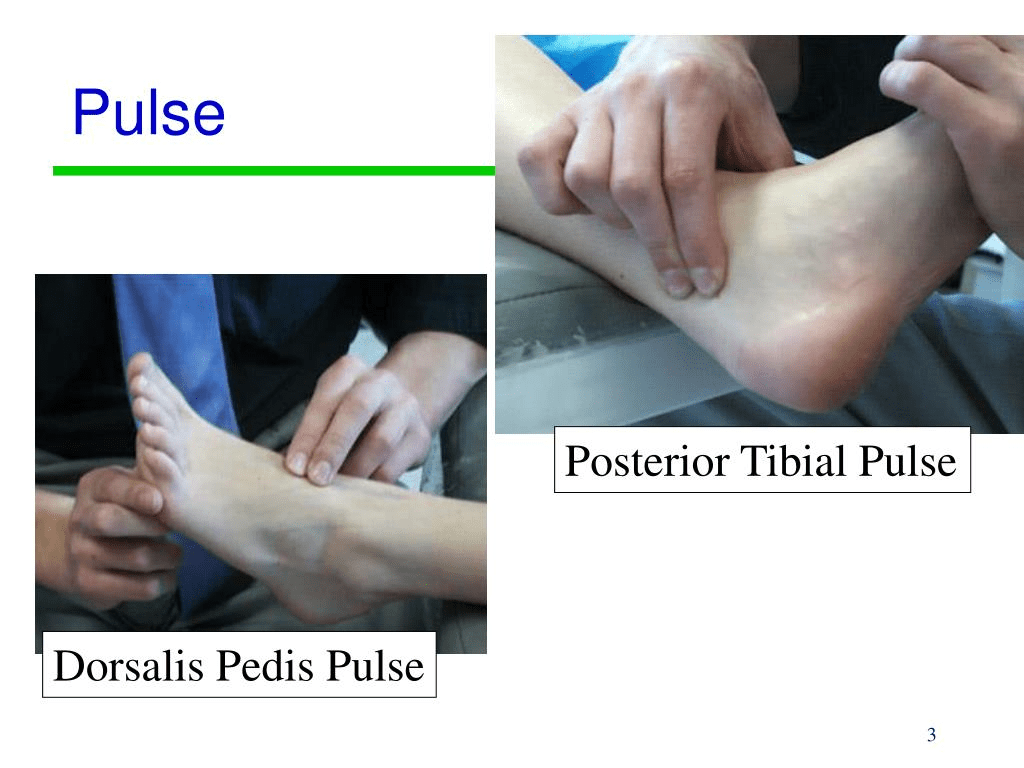
Dorsalis pedis
The dorsalis pedis pulse can be a bit variable. The most important thing is that it lies somewhere just lateral to the extensor hallucis longus, but may be over the cuboid bones or between the first and second metatarsals.
Because of this variation, when serial exams are required (such as with vascular surgery or trauma to the extremity), once the pulse is found, an X is often drawn on the skin to mark its location.



Leave a comment